Ocular Wavefront Sensing
Our understanding of the optical quality of the eye is becoming more accurate with the ability to precisely measure the lower and higher order wave aberrations using ocular wavefront sensing techniques. Reliable measurements of the ocular wave aberration also make it possible to correct these aberrations to improve visual performance using advanced methods such as adaptive optics, laser refractive surgery, and customized optics. This page summarizes how the ocular wavefront aberration is measured.
- Shack-Hartmann wavefront sensor
- Wavefront sensing in eyes with abnormal corneal conditions
- Characterizing aberration structures of eyes with abnormal corneal conditions
1. Shack-Hartmann wavefront sensor
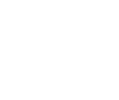
A Shack-Hartmann type wavefront sensor has been proven as a fast and objective way to measure the ocular wave aberration and is one of the most practical and robust techniques in a clinical setting. The Shack-Hartmann wavefront sensor works by essentially sending light into the eye and then making measurements on light that is reflected back out. More specifically, the incident light comes from a low-power, very narrow laser beam that is allowed to pass into the eye, where it is focused onto the retina. Light reflecting off of the retina becomes deformed as it passes through the eye's optics, crystalline lens and cornea. The aberrated wavefront emerging from the eye contains information about the optical defects it possesses. This wavefront is imaged onto a lenslet array which divides the aberrated wavefront into sections and images each section down to a point on a CCD camera. By measuring the distance that these spots move with respect to a reference, we can quantify the exact wavefront aberration present in the eye!
2. Wavefront sensing in eyes with abnormal corneal conditions
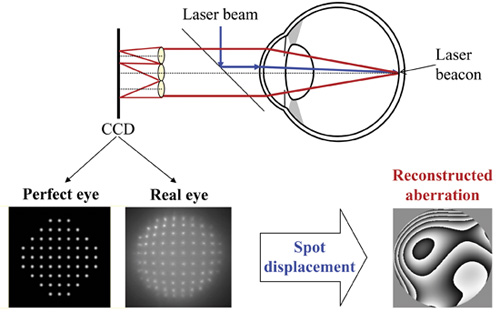
Although the Shack-Hartmann sensor works well for measuring normal eyes, limitations related to the amount of aberration the system can measure come into play with abnormal eyes (i.e. corneal transplant patients, people with keratoconus, etc). The amount of aberration the system is capable of measuring, is limited by the maximum displacement a single spot is allowed to move on the CCD camera. As diagrammed above, when a highly aberrated wavefront is incident upon the lenslet array, spots on the CCD camera may overlap or cross-over one another. When left with the spot pattern alone, it becomes impossible to map each spot to its corresponding lenslet. As a result, people with highly aberrated eyes are simply not measurable by the Shack-Hartmann wavefront sensor. We have developed a method for increasing the dynamic range of the Shack-Hartmann sensor so that highly-aberrated eyes can be measured. Our idea is to selectively block a portion of the lensets, allowing only a portion of them to image the wavefront at any given time. If we block every other lenslet, we increase the dynamic range by a factor of two, since the spots on the CCD camera can then be allowed to travel twice the distance. A metal plate, placed in front of the lenslet array, is used to do this. The metal plate can be moved to expose different lenslets. The data from each picture can be combined to include all of the information that would have been present in one picture without the plate.
3. Characterizing aberration structures of eyes with abnormal corneal conditions
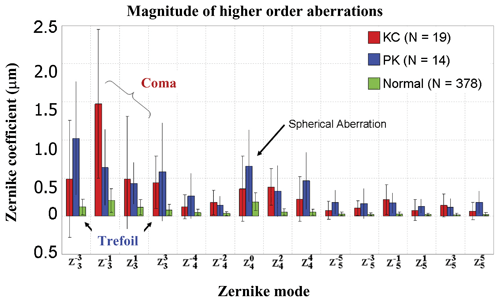
The ability to measure the abnormal corneal patients allows us to study the aberration structure of eyes with different corneal abnormalities. With the large dynamic range wavefront sensor described above, we measured large amounts of aberrations in 2 populations of eyes, namely those with keratoconus (KC) and those having undergone penetrating keratoplasty (PK). The keratoconic eyes exhibited 2.24 µm of higher order RMS on average for a 6mm pupil. As shown in the graph below, eyes with KC and PK have higher-order aberrations that are approximately 5.5 times more than what is typical in normal eyes. Vertical coma is the dominant higher-order aberration in people with KC, whereas PK eyes are dominated by trefoil, spherical aberration, and coma. These results indicate much poorer optical quality of eyes with abnormal corneal conditions and successful correction of these aberrations provides substantial improvements in vision beyond what is possible with conventional correction methods.